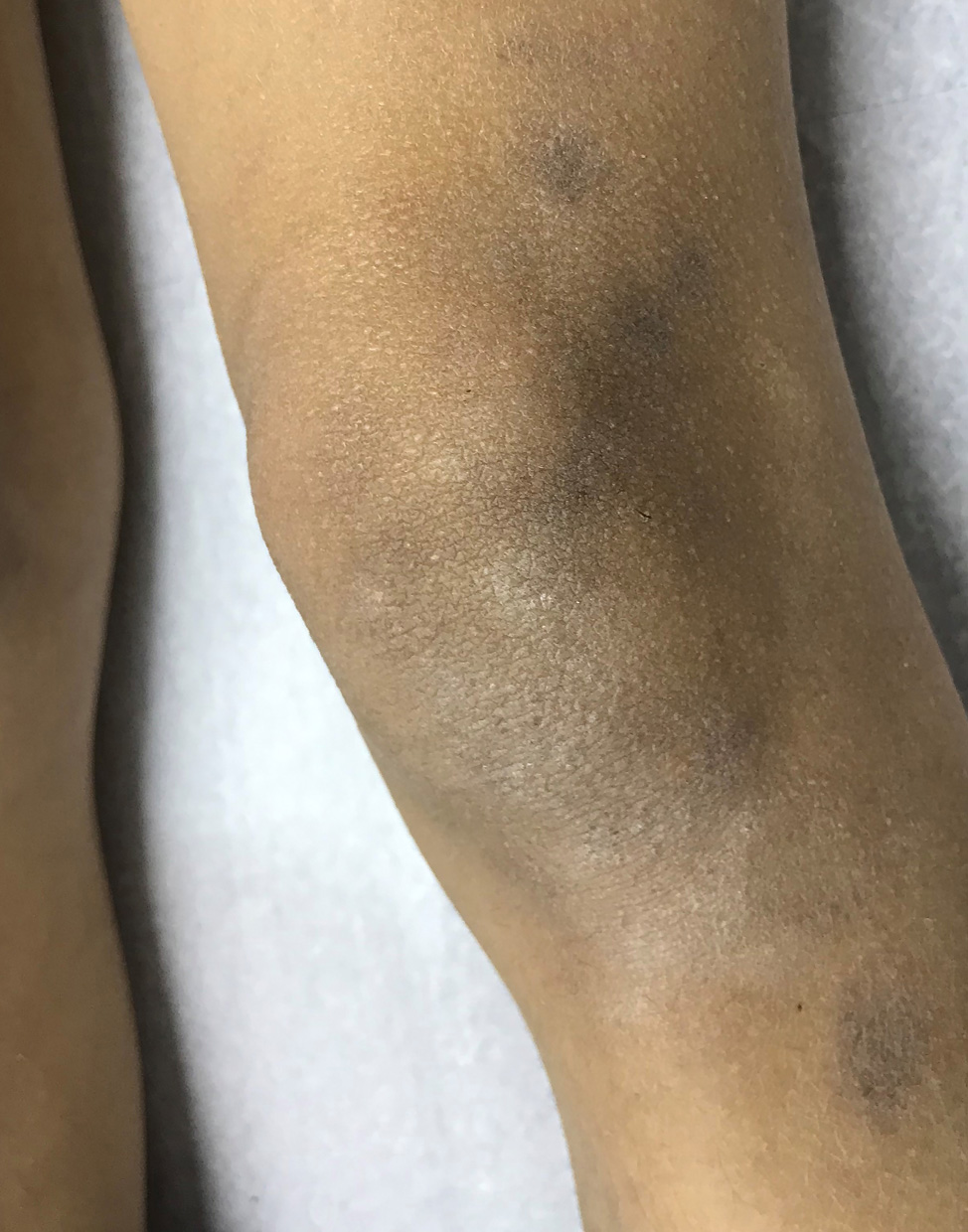
Lichen planus pigmentosus in a 7-year-old girl.
Downloads
DOI:
https://doi.org/10.26326/2281-9649.31.4.2294How to Cite
Abstract
LPP is a rare variant of LP that is infrequently encountered in children. In a retrospective analysis of 316 pediatric patients with LP, only nine (2.8%) were diagnosed with LPP (4). Similarly, in a recent retrospective study of 76 pediatric patients with LP in South India, only one (1.3%) was diagnosed with LPP (6).
It is commonly seen in middle-aged patients with high skin phototypes. LPP presents as chronic, acquired, violaceous to brownish-gray, oval macules, with poorly-defined borders (7). The lesions appear more frequently in the neck and face, but they can also affect the upper and lower extremities, and torso as well. LPP rarely affects the oral mucosa, scalp, palms, soles, and nails. Flexural involvement is seen in around 20% of cases with a concurrent photo-exposed distribution (5). LPP-inversus is a variant of LPP, limited to intertriginous and flexural areas, and sparing sun-exposed areas (3, 5).
A skin biopsy will confirm the diagnosis. The histopathology findings include hyperkeratosis and vacuolar degeneration of the basal layer, dermal band-like or perivascular infiltrate, and melanophages. Superficial pigmentary incontinence can be seen (7).
The main differential diagnosis of LPP is erythema dyschromicum perstans (EDP) or ashy dermatosis. EDP presents as non-pruritic, blue-gray macules and patches, with or without raised erythematous borders in photo-exposed areas and trunk. Histopathology reveals lichenoid features within the peripheral active border. A perivascular infiltrate and numerous melanophages can be seen. The clinical features and histopathology of LPP and EDP can overlap, so much so as to suggest that the two conditions can be part of the spectrum of a unique entity. Other differential diagnoses include post-inflammatory hyperpigmentation, pigmented contact dermatitis, fixed drug eruption, and urticaria pigmentosa, among others (2, 7).
LPP treatment is difficult, with limited results in most cases. The available topical treatments include medium to high potency corticosteroids, calcineurin inhibitors (mostly tacrolimus 0.1% ointment) and skin lightening creams containing hydroquinone and retinoids in conjunction with an anti-inflammatory treatment (3, 7, 9). Some Authors (3) recommend that in order to prevent steroid atrophy, corticosteroids should be used for a short period (2-4 weeks). Later on they could be followed by a calcineurin inhibitor over a longer period (3-6 months). In recalcitrant or widespread cases, systemic treatments with or without topical therapy can be used. They include oral corticosteroids, dapsone, and isotretinoin (7, 9, 10). The use of narrow band ultraviolet B (NB-UVB) phototherapy in LPP has been recently reported. Complete resolution of lesions was achieved after 20 exposures and no adverse effect was observed (1).